




When you are over 50, the eye’s lens deteriorates, causing changes such as blurred vision, hazy vision as if there is a film or fog, and distorted color perception. Screening for eye abnormalities is important because if cataracts are found, timely and appropriate treatment by an experienced ophthalmologist can help you regain clear, high-quality vision.

What is cataract surgery?
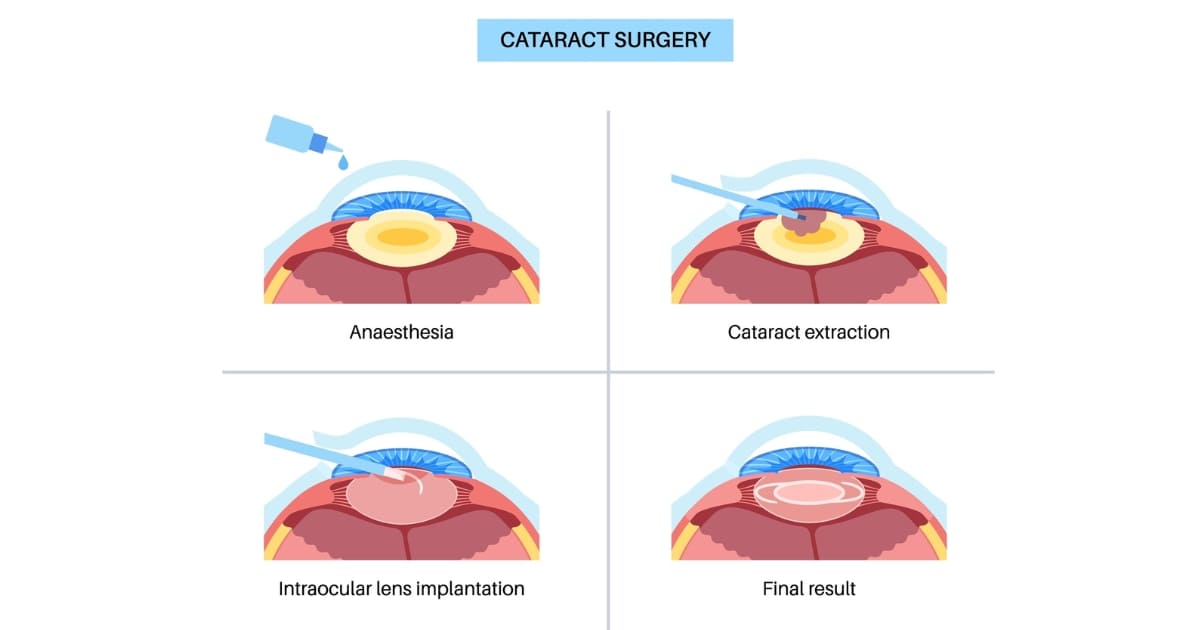
Cataract surgery is one of the most commonly performed eye surgeries. It involves removing the cloudy natural lens (cataract) and replacing it with an artificial intraocular lens (Intraocular Lens, IOL). Modern cataract surgery using ultrasound phacoemulsification (Phacoemulsification) not only restores clear vision but can also correct pre-existing refractive errors such as nearsightedness, farsightedness, astigmatism, or presbyopia, helping reduce dependence on glasses or contact lenses. However, the implanted IOL must be appropriately selected.
How many types of intraocular lenses are there?
There are 3 main types of intraocular lenses:
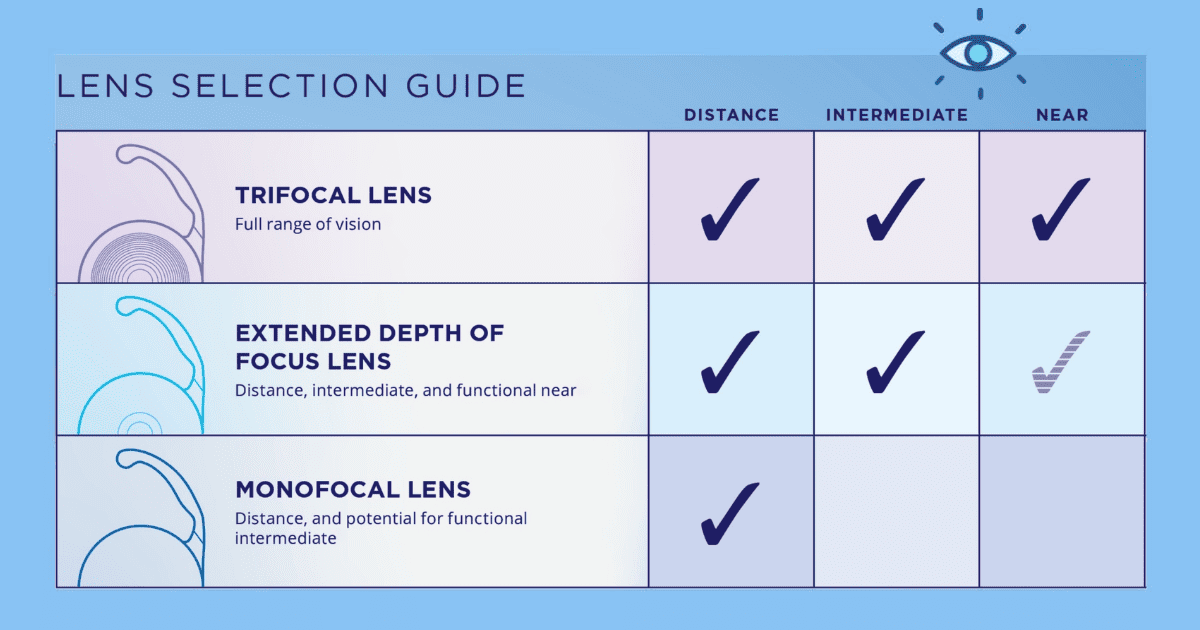
- Single-focus lens (Monofocal IOL) Provides clear vision at only one distance. It is usually chosen to be clear for distance in both eyes; near vision requires reading glasses. This is a standard and cost-effective lens with a lower chance of visual disturbances in low light. This group can also use a Customized Monovision approach, setting one eye for distance and the other for near.

- Multifocal lens (Multifocal IOL) Currently, this is designed for 3 focal distances (Trifocal IOL). The lens has multiple rings within its structure. After surgery, it allows clear unaided vision at multiple distances—near, intermediate, and far—reducing dependence on glasses and suitable for those who do not want to wear glasses. However, there is a chance of visual disturbances in low light; symptoms usually improve, but adaptation time varies by individual.

- Extended-range / extended depth of focus lens (Extended Depth of Focus IOL – EDOF IOL) Provides continuous vision across multiple distances, from far to intermediate, such as driving and computer use; near vision is somewhat adequate. It reduces dependence on glasses, but you may still need reading glasses for very small print. Newer designs in this group do not use multiple rings, resulting in a lower chance of visual disturbances in low light compared with multifocal lenses.

How to choose the right intraocular lens
What is an intraocular lens that corrects astigmatism like?
An intraocular lens that corrects astigmatism (Toric IOL) is for people with astigmatism caused by an uneven curvature of the cornea, similar to a rugby ball. This can be determined through an evaluation. The ophthalmologist may recommend adding an astigmatism-correcting lens as an additional option, chosen within the 3 main lens types mentioned above, to correct astigmatism and reduce the need for glasses to correct residual astigmatism after surgery—resulting in sharp vision according to the properties of the selected primary lens. When considering a toric IOL, the ophthalmologist primarily evaluates the corneal curvature or astigmatism in each eye, which may not directly correspond to the preoperative astigmatism prescription.

Normally, the cornea has a similar curvature in each axis, with a shape like a ball or basketball. But in people with astigmatism from uneven corneal curvature, the shape curves more like a rugby ball or an egg.
How many types of astigmatism-correcting intraocular lenses are there?
There are 3 types of astigmatism-correcting intraocular lenses:
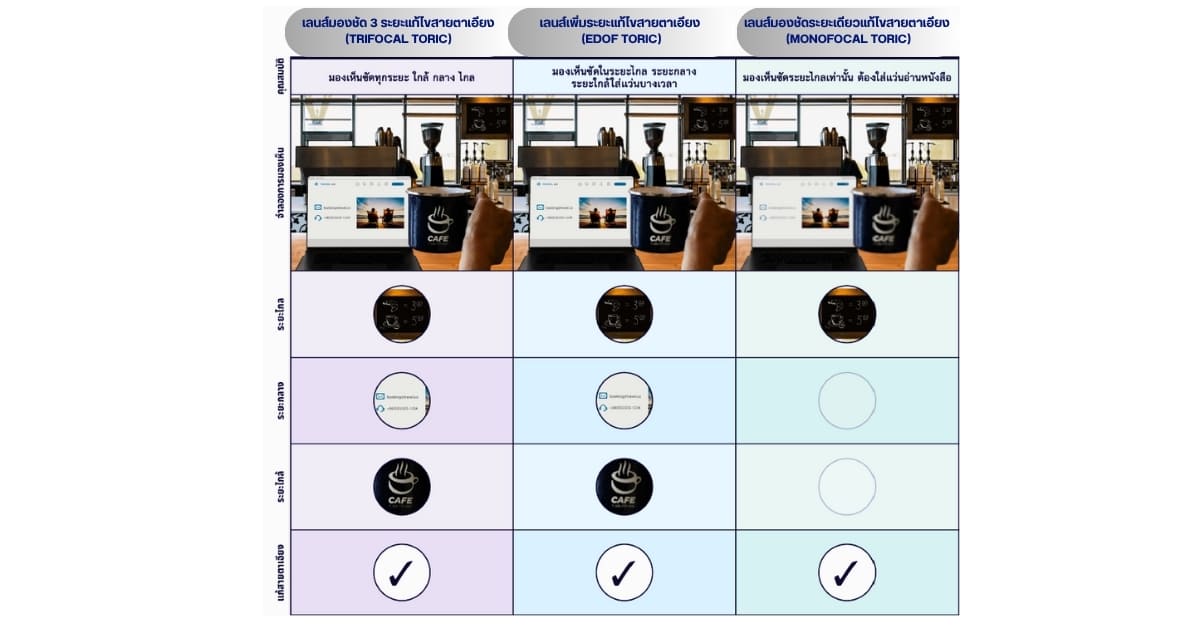
- Single-focus lens with astigmatism correction (Monofocal Toric IOL) Provides clear distance vision and corrects astigmatism, but near vision still requires reading glasses.
- Multifocal lens with astigmatism correction (Multifocal Toric IOL) Currently provides 3 focal distances with astigmatism correction (Trifocal Toric IOL) . After surgery, it can provide clear vision at multiple distances—near, intermediate, and far—reducing dependence on glasses.
- Extended-range / extended depth of focus lens with astigmatism correction (Extended Depth of Focus Toric IOL – EDOF Toric IOL) Provides vision at multiple distances, with clarity from far to intermediate, and some near vision; it also corrects astigmatism.
Preparing for cataract surgery
Most cataract surgeries use local anesthesia, so after surgery you can go home and do not need to stay overnight in the hospital. Preoperative preparation for cataract surgery includes:
- Wear comfortable clothing that is easy to put on and take off.
- Wash your hair and face before coming to the hospital.
- Upon arrival at the hospital, you will be prepared for surgery with anesthetic eye drops, pupil-dilating drops, and antiseptic drops before entering the operating room. Local anesthesia may be administered either as anesthetic drops or as an injection behind the eyeball (done in the operating room). If you are afraid of surgery, claustrophobic, or anxious, you can consult the doctor from the eye examination day and choose general anesthesia.
- Cataract removal using phacoemulsification takes about 15 – 30 minutes and is performed in a sterile main operating room. You will be awake during surgery but will feel relaxed and not in pain. You may see light and movement of light, or feel pressure on the eye, but it will not be painful like a cut from a blade.
- After cataract surgery is completed, you will rest in the recovery room for about 30 minutes and then can go home. If general anesthesia was not used, take medications as prescribed by the doctor, but you do not need to open the eye to instill drops yet. The doctor will schedule you to open the eye and have a postoperative eye check the next day, and then start using the eye drops.

How to care for yourself after cataract surgery
- Wear windproof glasses or sunglasses to prevent rubbing the eye and to prevent trauma to the eye.
- Before sleeping, cover the eye that underwent cataract removal with an eye shield to prevent rubbing or accidental impact during sleep for at least 2 weeks.
- Be careful not to subject that eye to severe direct impact.
- Absolutely avoid getting water into the eye for the period specified by the ophthalmologist (at least 2 weeks).
- Prevent germs from entering the eye and clean around the eye by wiping with saline and cotton twice a day instead of washing your face, strictly following the method recommended by the ophthalmologist.
- Avoid washing your face and washing your hair by yourself. You should lie on your back and have someone else wash your hair, and keep your eyes closed while your hair is being washed to prevent water splashing into the eye.
- Attend every scheduled follow-up eye appointment with the ophthalmologist, such as 1 day, 1 week, 1 month, 3 months, 6 months after surgery, and annually thereafter.
- Do not lift heavy objects. Be cautious about coughing, sneezing, or straining hard during the first 1 month after surgery.
What side effects may occur after cataract surgery?
- In the early period after surgery, be cautious about infection, which is rare but dangerous. Using eye drops and maintaining strict eye hygiene can greatly reduce this risk.
- Macular swelling can occur after surgery, typically beyond 1 – 2 weeks postoperatively, causing blurrier vision or distorted images. It can be treated and can return to normal.
- Long after cataract surgery, the lens capsule may become cloudy years after implantation. Vision that was clear soon after surgery may gradually become somewhat hazy. An ophthalmologist can resolve this quickly and easily without pain using a laser (Yag Laser) to remove the cloudiness immediately, restoring clear vision as if newly operated.
Why treat cataracts at Bangkok Hospital
- Specialist ophthalmologists who are trained, highly skilled, and very experienced.
- Thorough preoperative evaluation with modern medical equipment and a multidisciplinary team.
- New-generation intraocular lens technology designed to meet individual needs.
- Care at every step—from evaluation and surgery to postoperative follow-up.
More than cataract treatment,
it is about restoring the quality of vision so you can return to living life as you”
Which hospital specializes in cataract treatment?
Eye Center, Bangkok Hospital is ready to perform cataract surgery with intraocular lenses that suit your lifestyle, delivered by a highly experienced team of specialist ophthalmologists and a multidisciplinary team providing close consultation and care, supported by modern surgical equipment to restore strong eye health for every sight.
Doctors specializing in cataract treatment
Dr. Tarinee Sa-Ngiampornpanit Ophthalmologist specializing in cornea and refractive surgery, cataracts, Bangkok Hospital
You can click here to make an appointment by yourself.





