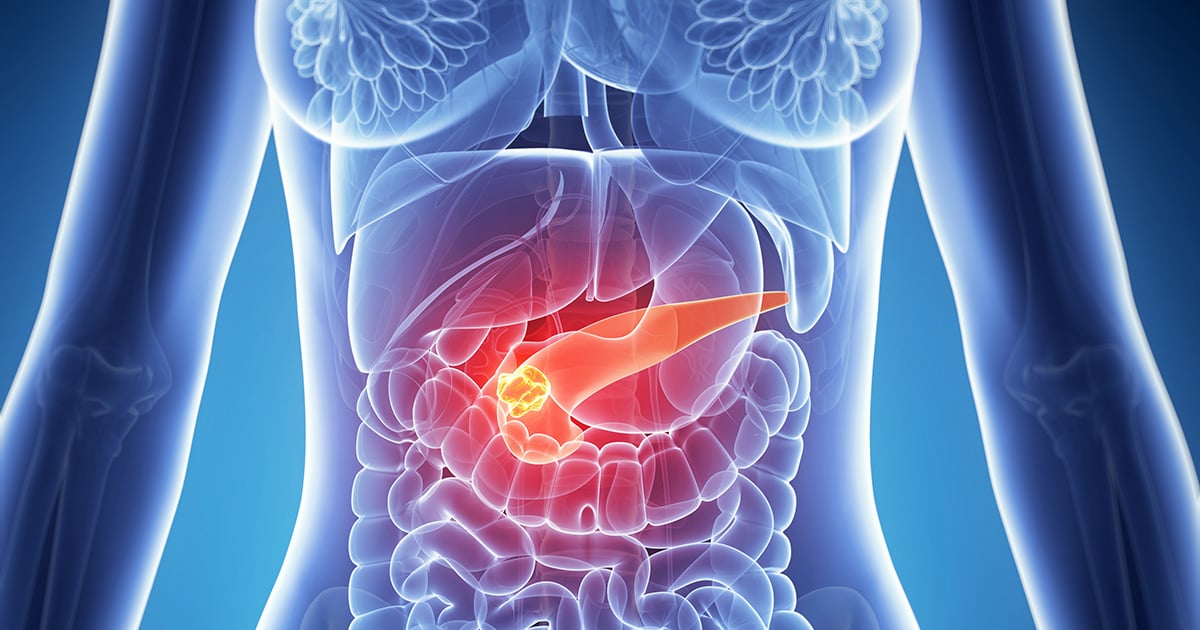
Types of pancreatic mass
Based on the histological characteristics of the mass, pancreatic mass can be generally categorized into solid pancreatic masses and pancreatic cysts described as fluid-filled sacs that form in the pancreas. Solid pancreatic masses without evidence of underlying pancreatic disease are usually identified as incidental lesions on abdominal imaging performed to evaluate nonspecific abdominal pain or for other indications. Most of these lesions are not related to the symptoms that led to the imaging. Both solid pancreatic masses and pancreatic cysts are usually discovered by ultrasonography or computerized tomography (CT scan).
- Pancreatic solid masses: If solid mass is detected in the pancreas, differential diagnosis is further required to determine whether it is benign (non-cancerous) or cancerous tumor. Detected masses could be diagnosed with a wide range of pancreatic diseases, extending from pancreatic mass lesion caused by pancreatitis (inflammation in the pancreas), pancreatic neuroendocrine tumor (PNET –a group of endocrine tumors arising in the pancreas), intrapancreatic accessory spleen (a benign condition in which a small nodule of splenic tissue is found in the pancreas) to pancreatic cancer.
- Pancreatic cysts: The characteristics of pancreatic cysts can be used to make a primary diagnosis. However, additional investigations e.g. endoscopic ultrasound (EUS), magnetic resonance imaging (MRI) or magnetic resonance cholangiopancreatography (MRCP) might be considered to obtain confirmatory diagnosis. In some cases, pancreatic cysts can be benign neoplasm which is not associated with cancer, such as serous cystadenoma (SCA) and pancreatic pseudocyst. Nevertheless, certain types of pancreatic cyst might tend to progress to cancerous conditions e.g. intraductal papillary mucinous neoplasm (IPMN), mucinous cystic neoplasms (MCN) and solid pseudopapillary epithelial neoplasms (SPEN).
Detected pancreatic masses
In case that pancreatic masses are discovered during regular health check-ups without any related sign and symptom, confirmatory diagnosis and treatment plans should be made by expert surgeon specialized in Hepato-Pancreato-Biliary (HPB) surgery. Nonetheless, if patients have exhibited relevant signs or symptoms, treatment plans will be discussed by gastroenterologist or specialized surgeon in that particular field.
Pancreatic masses: benign tumor vs. pancreatic cancer
As mentioned earlier, a wide spectrum of benign and malignant diseases can produce a mass in the pancreas. It can be either solid tumor (e.g. ductal adenocarcinoma, chronic pancreatitis, endocrine tumor) or a cystic lesion (e.g. cystic neoplasm, true cyst or pseudocyst). The most important question is whether or not it is a benign tumor or cancer. This question often causes anxiety and concerns to the patients. Diagnosis can be made based primarily on imaging results, signs and symptoms as well as individual conditions e.g. age, gender and underlying diseases. In fact, medical counseling with specialists to determine appropriate treatment plans is essentially important, resulting in effective outcomes in a timely manner.
Treatment of pancreatic masses
Selected approaches to treat pancreatic masses are principally determined by confirmatory diagnosis and patient’s symptoms. Depending on different diagnosis, treatments include:
- Benign solid masses without any symptom: In most cases, no treatment is required. However, frequent follow-up every 6-12 months is highly advised in order to monitor disease progression.
- Benign solid masses with clinical symptom(s): Treatment options depend mainly on presenting symptoms. For instance, if patient is present with jaundice, endoscopic retrograde cholangiopancreatography (ERCP) might be considered for biliary drainage without surgery.
- Large pancreatic cysts resulted from pancreatitis, causing the compression of adjacent organs: Endoscopic interventions might be performed. If inapplicable, surgery can be considered.
- Solid masses / cysts that are prone or confirmed to be malignant: If appropriate, pancreatic resection or pancreatectomy –the surgical removal of all or part of the pancreas might be performed, especially for curative disease management.
Pancreatic surgery and complications
Categorized by the affected part of the pancreas, pancreatic resection or pancreatectomy can be performed at two main locations: pancreatic head (pancreaticoduodenectomy or PD) and pancreatic body and tail (distal pancreatectomy or DP).
- The surgery of pancreatic head (pancreaticoduodenectomy)
Pancreaticoduodenectomy, also known as a Whipple procedure is a complex surgery to remove the head of the pancreas, the first part of the small intestine (called duodenum) and the distal part of bile duct.
This procedure is used to treat tumors and other disorders of the pancreas and bile duct. It is the most often used surgery to treat pancreatic cancer that is confined to the head of the pancreas. This procedure often consumes time since it involves resection (to remove pancreatic head) and anastomosis ( to reconnect the remaining organs including pancreas, biliary tracts and small intestine), allowing patients to digest food normally after surgery. This procedure is a difficult and demanding operation. It might develop serious risks and complications, ranging from 10% to 40%, depending on complication types and severity. However, this surgery is often lifesaving, particularly for patients with pancreatic cancer. Due to innovative approach and expertise, the death rates from surgery drop drastically, only to 1% to 5%. - The surgery of pancreatic body and tail (distal pancreatectomy)
Distal pancreatectomy is a procedure in which the tail and/or portion of the body of the pancreas are removed, excluding the head. It is considerably less complex. However, higher risks of pancreatic leak have been reported in distal pancreatectomy, compared to pancreaticoduodenectomy. In addition, patients who undergo pancreatectomy are at increased risk for developing a form of new-onset diabetes.
Surgical approaches
There are two main surgical approaches: open pancreatectomy and laparoscopic pancreatectomy which is a minimally invasive surgery. The location of affected part of the pancreas is used to appropriately select surgical technique. To surgically remove pancreatic body and tail, without contraindication, laparoscopic distal pancreatectomy might be preferred. However, if the mass is located at the pancreatic head, open surgery as a conventional approach remains the first line. Laparoscopic pancreaticoduodenectomy might be considered if conducted by highly experienced and well-trained surgeons. In addition, laparoscopic pancreaticoduodenectomy is a relatively new procedure that takes longer operative time due to high degree of difficulty and complexity. Besides the expertise of surgeon, this procedure requires cutting-edge technology and advanced facilities available in certified hospitals.